
|
|
||
|
Simply Silver Intubation is relatively common; unfortunately, so too are infections.
|
||||||
|
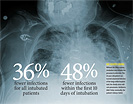
Traditional intubations increase the risk of infection for critically ill and severely injured patients. Research by Marin H. Kollef, MD, and colleagues, shows that use of silver-coated tubes dramatically drops infection rates.
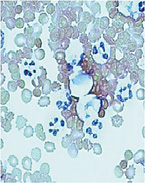
Cells from the lungs of a patient with ventilator-associated pneumonia. White blood cells (large cells with blue nuclei) in the sample suggest infection. Later tests showed that the sample included bacteria called Klebsiella — some strains of which have become antibiotic resistant. |
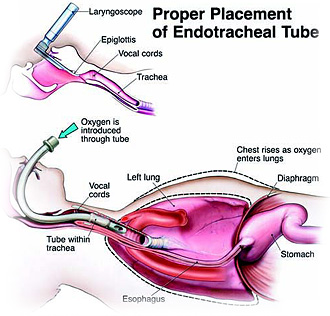
Sometimes the simplest solutions are the best. Doctors and nurses try many things to keep pneumonia from striking critically ill patients on artificial ventilation. They rinse patients' mouths with antiseptics. They elevate the heads of their beds to help keep air passages clear. They purge ventilator circuits of collected fluids. They take care that patients don't regurgitate stomach contents. They diligently wash their hands. But pulmonary specialist Marin H. Kollef, MD, and colleagues tried a different approach. Working with a device manufacturer, they armed breathing tubes used during ventilation against pathogens by coating them with antimicrobial silver. In a recent study, they showed an almost 50 percent reduction in ventilator-associated pneumonia as a result. That could save a lot of lives and lessen the physical and financial burden of lung infection — all without giving extra duties to busy medical staff members. Artificial ventilation requires tracheal intubation — insertion of an endotracheal tube into the windpipe. Patients needing long-term intubation (more than a day) include those in intensive care units after a cardiac arrest, trauma or emergency operations, or patients who have an exacerbation of their emphysema, asthma or cystic fibrosis. The endotracheal tube goes through the mouth and vocal cords and into the windpipe, or trachea, which leads to the lungs. It ensures that patients can get air, and it can be attached to a mechanical ventilator when necessary. Unfortunately, long-term tracheal intubation often leads to pneumonia. When tubes are placed in an emergency situation, it's common for microbes to be introduced into the lung. Also, intubation interferes with coughing and with the ability of airways to naturally sweep out particles. It also can injure the trachea lining. All that can give pathogens a direct conduit to the lungs.
Ventilator-associated pneumonia occurs in up to two of every 10 patients who are mechanically ventilated for more than 48 hours, according to a recent analysis. It causes excess expense along with substantial suffering and death. Hospital stays can double in length, and on average more than $40,000 extra is spent for ventilated patients who contract pneumonia. Some experts estimate that up to two fifths of patients with ventilator-associated pneumonia will die. Hospitals routinely institute a suite of procedures aimed at preventing any harmful microbes that might be in patients' mouths and gastrointestinal tract, in the air, on equipment or on caregivers' hands from getting in the breathing tubes. "The problem is that it can be very difficult to maintain many of the preventative interventions 24 hours a day for critically ill patients," says Kollef, professor of medicine in the Division of Pulmonary and Critical Care Medicine. "And even though we use such techniques and keep our rates as low as we can, infections still happen." So Kollef and colleagues approached medical device manufacturer C.R. Bard Inc. to suggest working together on a way to reduce ventilator-associated pneumonia. The result of their collaboration — an endotracheal tube that's basically immune to pathogens. It's coated inside and outside with a polymer containing silver ions. Silver ions kill many kinds of bacteria, viruses and yeasts, and silver is garnering more interest lately because some microorganisms have developed resistance to standard antibiotics. Antimicrobial silver can now be found in a wide range of applications such as surfaces and equipment used in food processing, bandages and ointments for wounds, washing machines that release silver into the wash water and even silver-coated computer mice and keyboards.
A purple cap distinguishes the frosted tube with the silver coating — nearly invisible but critical for preventing infections. "Silver particles diffuse out of the coating of the endotracheal tubes to the surface environment," Kollef explains. "That creates zones of inhibition where microbes are killed. The silver also helps prevent formation of biofilms, which colonies of microorganisms build to protect themselves. And some of the silver probably makes its way into the lung where it could also have an antibiotic effect." The silver-coated endotracheal tube is structurally identical to a typical tube, so its adoption would not require any change in standard intubation procedures. Early tests showed that in both animals and humans the silver-coated tubes were safe. In animal tests, the tubes decreased the number of bacteria in airways of the lung and reduced pneumonia and lung injury. The tubes lessened the amount of bacterial growth in patient's lungs and didn't increase the amount of silver in the blood. With such evidence in hand, Kollef and his colleagues devised a large, randomized multicenter clinical trial, the North American Silver-Coated Endotracheal Tube Study (NASCENT), which investigated whether the tubes would reduce ventilator-associated pneumonia in patients who needed mechanical ventilation for 24 hours or longer. The study included researchers from 11 centers around the United States and one in Germany. The silver-coated tubes reduced cases of ventilator-associated pneumonia by 48 percent in patients intubated for more than 24 hours and less than 10 days. Generally, three-fourths of patients have their endotracheal tubes removed before 10 days. In patients who needed endotracheal tubes for longer than 10 days, the reduction was 36 percent. The study also showed that in patients with silver-coated tubes, fewer cases of pneumonia were caused by highly drug-resistant bacteria, including methicillin-resistant Staphylococcus aureus (MRSA), which is unsusceptible to broad-spectrum antibiotics. "Ventilator-associated pneumonia is often caused by antibiotic-resistant pathogens," Kollef says. "These pathogens are becoming increasingly common in hospitals. It's a big problem; we are facing infections for which we have no good treatments." And, even when an infection can be treated with antibiotics, it takes a physical toll on the patient. Silver kills microorganisms by binding to the proteins and genetic material so that the pathogen can't function or reproduce. Microbes very rarely, if ever, acquire resistance to silver. Furthermore, silver has no side effects in people, and allergic reactions to the metal are rare. The silver-coated tubes will be more expensive than uncoated tubes — costing around $80 compared to $2 — but that cost is easily recovered if the silver-coated tubes can reduce the number of cases of pneumonia, Kollef points out. "This is the beginning of a new era of technologies to prevent microbial biofilms and infections," Kollef says. And other advances are on the horizon. "The silver-polymer coating will most likely be applied to tracheostomy tubes as well, and the tubes will also become available for use in pediatric medicine. In the future, we are going to see other types of coatings for other purposes used in devices that come in contact with the body."
|
|||||