
|
|
||
|
Avoiding diabetic foot ulcers One Step at a Time Common medical wisdom says diabetic complications often lead to foot amputation. But "smart shoes" and surgeries could minimize what was once thought inevitable.
|
|||||||
|
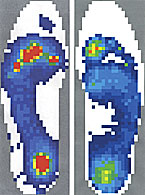
Lacking sensation in their feet, patients with neuropathy can't feel trouble when it starts. The top color images show external pressure points (red) corresponding to internal bone deformities—and reveal hot spots for ulceration. Below, these side views likewise show pressure points beneath a diabetic foot; the control image shows healthier pressure distribution.
High stress areas on a diabetic's foot are shown left in red, compared to the healthier foot on the right which indicates more even weight distribution.
The "smart shoe" features a sensory pad wired to a data recorder. |
DIABETES IS A GROWING HEALTH PROBLEM IN AMERICA, and more people with diabetes means more people with foot ulcers, a common side effect of the disease. It’s an unfortunate complication that often leads to amputation. Now, research conducted at the School of Medicine may keep people with diabetes on their feet. People with diabetes are 15 times more likely to undergo amputation than members of the general population. Peripheral neuropathy, a loss of feeling in the extremities, renders these individuals unaware of sores that develop on their feet until the wound becomes infected. Then, because of other diabetes-related complications, the infection often defies healing and eventually leads to amputation. “The overwhelming majority of nontraumatic amputations in the United States are due to diabetes—about 85 percent,” says David R. Sinacore, PT, PhD, associate professor of physical therapy and of medicine. In a series of groundbreaking research projects, Sinacore, Michael J. Mueller, PT, PhD, associate professor of physical therapy, and Jeffrey E. Johnson, MD, associate professor of orthopaedic surgery, have concluded that these amputations are avoidable. They believe that with some imaginative techniques and high-tech devices, foot ulcers can be healed and even prevented. Amputation resulting from diabetes complication is a problem that is difficult to overstate, not just for individuals who have lost limbs, but for the nation. The cost of treating these foot ulcers is about $5 billion annually. At any given time, there are 800,000 ulcers on American feet, with 200,000 new cases each year. Physical therapists Mueller and Sinacore focus on neuropathic ulcers, those that develop because patients can’t feel pressure on the foot. Under the neuropathy umbrella, various deformities of the foot are often the culprits in skin breakdown. A bunion, for instance, presses against the shoe —first raising a blister and then becoming an open wound susceptible to infection. Healed wounds are likely to recur. “This population
is characterized by having ulcerations. They close, reulcerate, and then
open again,” Sinacore says. “It’s hard to heal these things
and keep them healed.” “David and Michael have brought a real shift in the treatment of diabetic foot ulcers,” says Susan S. Deusinger, PT, PhD, director of the School of Medicine’s Program in Physical Therapy. “We used to ask: ‘How can we manage amputations?’ Now, we are working to prevent amputations. These are life-and-limb-saving strategies.” A dozen years ago, the researchers published results from a clinical study that showed the effectiveness of total contact casting in healing foot ulcers. By distributing weight evenly over the surface of the foot, the cast takes excessive pressure off the ulcer. Research showed that 95 percent of neuropathic ulcers will heal using this method. Unfortunately, once the cast is removed, a large percentage reulcerate.
Michael J. Mueller, PT, PhD, and David R. Sinacore, PT, PhD, along with graduate student Katrina Maluf, review data collected from the sensory shoe. Now Mueller and Sinacore are looking at some new ways to tackle the ulcer problem. One key to their success is the interdisciplinary nature of their work: Orthopaedic surgeon Johnson heads the clinical team and refers his patients for physical therapy study; faculty from the Departments of Radiology, Electrical Engineering and Mechanical Engineering also are active participants. Together with Johnson, Mueller and Sinacore began looking at other approaches to prevent or heal wounds. One that has yielded good results is a surgical technique to lengthen the Achilles tendon. In an NIH-funded trial, Johnson performed a procedure in which he lengthened the heel cord in a group of diabetic patients with foot ulcers. The trial has shown that the reulceration rate for those patients who underwent surgery was only one-fourth that of a control group. The reason for that, the team concluded, was that patients with the lengthened heel cord had more range of motion at the ankle and a greater percentage of pressure on the heel. They then pushed off less with the ball of the foot, taking pressure off the forefoot where ulcers are most common. Johnson notes, however, that in a few cases the surgery weakened the calf muscle excessively so that patients then developed ulcers at the harder-to-heal back of the foot. Therefore, calf muscle strengthening and appropriate diabetic footwear are essential to the success of this treatment. Enter computer technology. Mueller, Johnson, and members from the Department of Radiology, Douglas D. Robertson Jr., MD, PhD, and engineers Kirk Smith and Paul Commean, have developed methods for visualizing and measuring foot structure from spiral X-ray computed tomography (SXCT). Now, in a second major NIH-funded project, they are combining SXCT imaging methods and the pressure analysis into a mathematical model to quantify the links between internal structures and external pressures on the foot.
Mathematical models are a promising avenue of investigation. “We just had a research retreat with Ricardo L. Actis, DSc, and Barna A. Szabo, PhD, in the Department of Mechanical Engineering to plan a finite element analysis of the foot,” Mueller says. “The computational model will combine the structure of the foot, the material properties of its soft tissue and the pressure on the bottom of the foot.” Using these models, the researchers hope to determine how the foot responds to stress, allowing for the development of software that would apply computer-assisted design technology to the production of orthotic devices and custom shoes. Mueller adds: “In four years we should be able to indicate the optimal characteristics of the insole—the shape, the location of different kinds of loading patterns, and the material properties.” In another project, also funded by the NIH, the team worked with Robert E, Morley Jr., DSc, associate professor of electrical engineering, to develop a data collection unit (DCU) to gather information from sensors in a shoe. The DCU measures, records and analyzes a variety of conditions, including vertical force and temperature and humidity inside the shoe. Via a radio signal, it provides feedback to a unit the patient wears on a belt. Though now the DCU straps to the calf, Joseph Klaesner, PhD, a biomedical engineer in the Program in Physical Therapy, has obtained funding to miniaturize it so it can fit inside the shoe. Eventually, the team plans to add audible or pulsing alarms to signal risky conditions. “We’re calling this the ‘Get Smart’ shoe,” Mueller says with a grin. “We’re hoping to have something that the patient can wear for an extended period of time that will collect information and provide feedback when the patient is at risk for skin breakdown.” A signal would alert patients to get off their feet. People with diabetes will not be the only beneficiaries of the research. The “smart” shoe, Mueller says, “will be useful for anyone who needs ongoing feedback. This device would be like a virtual physical therapist.” The obese or elderly, for instance, could use it to prompt exercise. “It takes 10,000 steps a day to be healthy, to reduce the risk of gaining weight and having high blood pressure,” Sinacore notes. “These kinds of devices could lend themselves to meeting those prescriptive recommendations for health.” All of the approaches to heal open ulcers, however, are concerned fundamentally with adjusting pressure on the unfeeling foot. “If pressure is the key thing that breaks the skin down and keeps the ulcers open, then if we can reduce the pressures they should be able to heal and heal very quickly,” says Sinacore, who currently is leading the team in an NIH-funded clinical trial to determine the optimal methods of reducing pressure using total contact casting or removable walking boots. All of the research projects that change the care of the
feet of diabetic patients could potentially save thousands of limbs and
millions of dollars in health care costs.
|
||||||