
|
|
||
| The Way to the Heart Catheterization offers less invasive treatments
|
|||||||
|
The Washington University cardiology team at Barnes-Jewish Hospital has one of the lowest restenosis (the reclogging of the artery) rates in the country,with an average of just 16 percent of all patients returning for further treatment.
“It is absolutely astounding how much progress we've
made in such a short period of time.”
|
A PHYSICIAN SKILLFULLY THREADS a thin catheter over a wire and through an artery, inching toward the heart of a patient whose health hinges on the procedure’s outcome. Following the catheter’s tip via an X-ray monitor, the cardiologist wields tiny tools to forestall life-threatening coronary disease. The journey, from a small puncture site in the thigh through the body’s inner recesses to the vital heart, has taken modern cardiology 50 years to envision, refine and put to effective use. Roots of intervention In 1929, a German surgical trainee named Werner Forssmann inserted a catheter into a vein in his arm and guided it into the right side of his heart. He then walked to the X-ray room and became the first person to prove, using imaging, that catheters could be used to study the living, human heart. His intrepid experiment got him fired; later, in 1956, it earned him a Nobel Prize. By that time, the use of catheters was revolutionizing the state of cardiac diagnosis by measuring the amount of oxygen in the blood and locating clogged arteries. Two decades later, Dr. Andreas Grunzig went a step further, using balloon catheters to treat heart patients. With that, the non-surgical treatment of heart conditions — interventional cardiology — was born.
Cardiac cath can: Expand and clear passages, insert a tube to hold an artery open, place long-acting drugs for continued treatment, attack a little tissue to rescue the heart, plug a hole in the heart. Opening the way The rapid evolution of interventional cardiology over the past 30 years can be traced by the progression of treatment for coronary artery disease (CAD), a condition in which the heart’s main blood vessels become narrowed or clogged by the buildup of plaque. According to the American Heart Association, more than 13 million Americans have CAD, and it remains the leading cause of death in this country. Before the use of catheters, patients whose conditions did not improve with drugs typically underwent surgery in which the diseased artery is bypassed by a blood vessel from the leg, arm or chest. The operation not only harvests a blood vessel from another part of the patient’s body, it also necessitates making a 12- to 18-inch incision in the chest — both of which result in scarring and postoperative pain. The most dangerous aspects of bypass surgery, however, are the use of general anesthetic and a heart-lung bypass machine to divert blood away from the heart during the operation, temporarily stopping the heart from beating. The catheter-based alternative, percutaneous transluminal coronary angioplasty (PTCA), avoids those issues. Interventional cardiologists typically insert the catheter into a blood vessel in the groin and watch X-ray images as they maneuver it through the artery’s natural twists and turns. When it reaches the clogged portion of a coronary artery, a balloon on the tip of the catheter is inflated, compressing plaque buildup against the blood vessel’s wall and reopening the passage to blood flow. The advent of this less invasive approach has revolutionized
both the treatment and prognosis of CAD. More than 1 million PTCAs will
be performed in the United States in 2004, surpassing the number of bypass
operations by more than 50 percent.
John M. Lasala, MD, directs the School of Medicine’s cardiac catheterization laboratory. Keeping it open In 1989, John M. Lasala, MD, medical director of the School of Medicine’s cardiac catheterization laboratory, witnessed a seminal moment in the history of heart care. Then a cardiology fellow at Yale University, Lasala observed as his mentor Henry Cabin, MD, used a small metal cylinder to prop open a patient’s clogged artery — one of the first times the device, called a stent, was used in the United States. “There was silence in the room,” recalls Lasala, who also is director of interventional cardiology at Barnes-Jewish Hospital. “Henry said, ‘You’re looking at the future.’ It literally sent a shiver up my spine.” His mentor was right. While balloon angioplasty generally succeeds in opening arteries, about 30 to 50 percent of blood vessels become reclogged, or restenosed, within months of the procedure. Furthermore, balloon results were acutely unstable, requiring urgent bypass surgery in 3 to 7 percent of cases. As Lasala witnessed first-hand in 1989, the addition of stents — short narrow metal tubes often in the form of mesh- — significantly alleviates both problems. These small cylinders fit around the balloon and expand as it inflates. The stent then remains in place after the balloon and catheter are removed, serving as scaffolding and holding plaque buildup at bay. Since the Food and Drug Administration (FDA) approved the first stents in 1994, the number of patients whose arteries become reclogged is about half the rate of traditional balloon angioplasty. The Washington University cardiology team at Barnes-Jewish Hospital has one of the lowest restenosis rates in the country, with an average of just 16 percent of all patients returning for further treatment. But Lasala still isn’t satisfied. That’s why he’s been at the forefront of the most recent innovation in catheter-based CAD treatment: drug-coated stents. Lacing the mesh cylinders with low doses of drugs designed to slowly diffuse into the artery appears to further decrease the risk of restenosis. Lasala’s team was one of the key participants in research that led to the FDA’s landmark approval of a Johnson & Johnson stent in April 2003, the first federally approved drug-coated stent. “It is absolutely astounding how much progress we’ve made in such a short period of time,” Lasala says. “Our early results with drug-coated stents are almost too good to be true — restenosis rates have dropped to less than 5 percent, and we expect them to be even lower as we continue to smooth out the wrinkles. This may be the most important advancement in interventional cardiology this decade.”
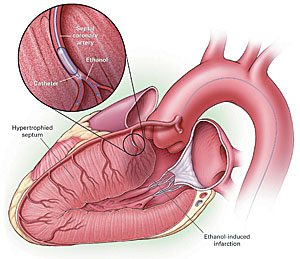
Tiny heart attack Along with such impressive results in treating conditions like CAD, catheter-based interventions have gone beyond clogged arteries to treat other serious heart conditions. One of the newer procedures, developed in the early 1990s
by a European scientist named Ulrich Sigwart, relies on an unlikely ally:
a heart attack. Patients with HOCM have abnormally thick heart muscles, particularly between the two lower chambers of the heart. The thickened muscle makes it more difficult for the heart to pump blood to the rest of the body, and its enlarged size obstructs the passageway through which blood normally flows. HOCM often affects very young individuals and is the leading cause of sudden death in athletes. Previously, the only option for treating HOCM patients who didn’t improve with drug therapy was to surgically remove a portion of the enlarged heart muscle. Using septal ablation, cardiologists inject 200-proof alcohol through a catheter into the branch of the artery that feeds the section of muscle obstructing blood flow. The alcohol causes a localized heart attack, killing an area of tissue about the size of a grape. Bach found it hard to imagine that this less invasive approach would help a patient so severely afflicted by HOCM that he could barely get out of bed. But it did. “The result was beyond what I ever expected,” Bach recalls. “Our patient’s condition was so extreme that I didn’t know if we could help him. But we did the procedure and the next day he was up and walking, feeling dramatically better. I’ve now seen that remarkable outcome re-iterated over and over again in many other patients.” Though septal ablation doesn’t actually cure the underlying condition, it does substantially relieve symptoms more than 90 percent of the time. For this reason, Bach’s team proceeds with cautious optimism and is investigating the long-term benefits of the procedure, as well as studying ways to improve the technique. In collaboration with Bruce D. Lindsay, MD, associate professor of medicine, Bach recently performed the first septal ablation for HOCM using a magnetically guided catheter. Instead of a wire, catheters used in the Magnetic Navigation System contain a magnetic tip, which is directed by a computer-controlled magnetic chamber positioned around the patient. The system, which was developed by St. Louis-based Stereotaxis, Inc., in collaboration with School of Medicine researchers, enables cardiologists to maneuver the catheter around particularly sharp twists in the arteries that are difficult to navigate with a traditional, wire-threaded catheter. On the horizon Washington University cardiologists also have been selected to test three catheter-based approaches to fixing leaky valves in the heart and are evaluating a catheter alternative to surgical treatment of a common birth defect called patent foramen ovale (PFO), a type of hole in the heart that is one of the main causes of strokes in people under age 55. “For the foreseeable future, there will always be
complex cases in which open-heart surgery is the best option for patients
with heart or blood vessel diseases,” Bach says. “But what’s
truly exciting — and the reason I went into interventional cardiology
— is that angioplasty allowed us to begin radically altering someone’s
condition without surgery. Now we’re extending that to a wider range
of diseases, like HOCM and treatment of valvular disease and PFOs. It
just keeps getting better.”
|
||||||