|
|
||
|
The Inner Turmoil of TOS Misunderstood syndrome responds to delicate surgery
|
|||||||
|
On the rebound from Thoracic Outlet Syndrome: Aaron Cook is back in the game following surgery by Robert W. Thompson, MD. |
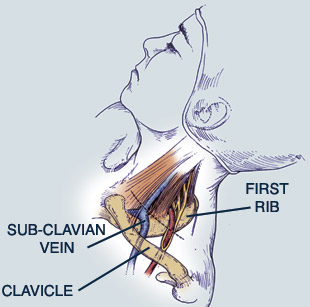
TWO YEARS AGO, when Aubrey Turvey first visited vascular surgeon Robert W. Thompson, MD, she was desperately in need of answers. For four hard years, she had bounced from one physician to another, trying to discover the cause of disabling pain above her collarbone and in her right arm. Standard tests came back negative, and finally one specialist suggested the pain was in her head. “That was a real slap in the face,” she says now. “I started wondering, ‘Could I be creating this?’” On the mound, he was short of breath and dizzy, his pitching speed slacked off and he gave up a series of hits before being pulled from the game. For Colorado Rockies pitcher Aaron Cook, his ordeal began during an August 2004 game against the Cincinnati Reds. Trainers discovered a low blood oxygen level and sent him to a Denver hospital where doctors dissolved dangerous clots in his lungs — but what was causing them? Two weeks later, he came to Thompson for treatment. Suffering from versions of the same condition, both Turvey and Cook were diagnosed with Thoracic Outlet Syndrome (TOS). In its neurogenic form, the kind Turvey had, TOS is difficult to diagnose and little understood. Some doctors even doubt its existence, because overt physical signs may not appear for years; eventually Turvey’s arm turned blue and felt cold to the touch. Venous TOS, the kind Cook had, is more easily recognized because it entails a blood clot that is visible in imaging studies. Thompson is a national expert on TOS in all its forms — including a third version, arterial TOS — and he is working to build a multidisciplinary TOS center at Washington University. But at one point, he knew little about it, because his surgical training in Boston barely touched on the condition. Only during a vascular surgery fellowship at the University of California-San Francisco, a center with long experience in TOS, did he begin treating several patients a week. All had the same story: a chronic, debilitating arm or neck condition that had baffled their physicians. “When I saw these patients several months after surgery, I found their lives had changed,” he says.“ They might still have some symptoms, but the majority had substantial improvement. It is tremendously satisfying to help return someone to a full and active life, especially from a condition that is so misunderstood.” Types of TOS While doctors once thought that patients with an extra cervical rib were more prone to neurogenic TOS, most now focus on the adjacent thoracic outlet space: a tight anatomic area bounded by the two scalene muscles and the first rib. In neurogenic TOS, an injury probably causes tearing and spasm in the scalene muscles, which become inflamed and scarred, irritating the adjacent nerves. In arterial TOS, the patient has developed an aneurysm of the subclavian artery in the neck; clots may break off and travel to the hand, which turns painful and numb. Venous TOS — sometimes called “effort thrombosis” — begins when the subclavian vein is pinched between the rib and collarbone, which leads to a vein injury. With repeated injuries, a cuff of scar tissue forms, narrowing the vein; pressure builds up behind it, and the body forms collateral vessels to handle the blood flow. But the obstructed vein still has some stagnant blood flow, prone to forming a clot; if this clot propagates, blocking the collaterals, the arm suddenly swells. Athletes like Cook may be especially vulnerable to such injury, but others who repeatedly use their arms overhead are also susceptible. In general, TOS occurs in young people: under age 45 in the neurogenic form and under age 25 in the venous and arterial kinds. In neurogenic TOS, perhaps three-quarters of all patients are women. Overall, the TOS population consists of 80 percent neurogenic cases, 15 percent venous and 5 percent arterial.
Former TOS patient Aubrey Turvey now works for Thompson explaining TOS to new patients. Surgical Solution Caught early, mild neurogenic TOS may respond to appropriate physical therapy. Aubrey Turvey, injured when she was thrown from a horse, initially received incorrect therapy that only exacerbated her condition. Later, she had the right kind of therapy, but it still did not help. She went to see Thompson. Both Turvey and Aaron Cook decided to undergo the delicate TOS surgery (see sidebar), which can range from three hours for neurogenic TOS and up to 12 hours in some cases of venous TOS. Some patients have dramatic results. “Those are the patients you dream about, who tell you in the recovery room that all their symptoms are gone,” says Thompson. “More often, we see a gradual improvement over four to six weeks, while patients undergo significant physical therapy.” To athletes, Thompson gives a chilling warning at the outset. “We say, ‘This is potentially a career-ending problem; now let’s see what we can do for you.’” Cook’s outcome was good. After September surgery, he could throw a little in spring training; by mid-season, he was in the starting rotation, and by late in the season he had a 7-2 record, with his manager proudly calling him their “man.” During that first visit to Thompson’s office, Aubrey Turvey learned that she had a physical condition — one that was treatable. “At that point,” she says, “I had been put on nearly every possible medication. I just started crying and said, ‘Thank God, somebody finally believes me.’” Two months following surgery, she and her mother came back to Thompson’s office for a follow-up visit. “We both cried again, because we were so thankful that he had given me my life back.” Now Turvey works as a research assistant, videographer and photographer in Thompson’s office and tells new patients about her experience. “So many of these people have gone through exactly what I did,” she says. “There is an important need for education about Thoracic Outlet Syndrome, not just for patients but also for physicians. Medical professionals need to be able to recognize this condition and get patients to the right place at the right time.”
|
||||||