|
|
||
|
What's Next for HIV 25 years and counting
|
|||||||
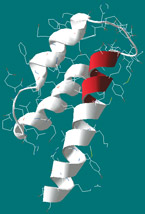
Understanding how HIV weaves its genetic material into a host cell's DNA can help scientists develop new integrase inhibitor drugs. Lisa Mahnke, MD, PhD, and Lee Ratner, MD, PhD, studied a West African strain called HIV-2 and revealed domains shown in red that are critical for carrying the viral genome into cell nuclei. |
Twenty-five years after the first Centers for Disease Control report describing a new infectious disease afflicting the immune system, HIV infection is no longer the automatic death sentence it once was. Still, the virus remains a life-changing and potentially deadly burden, a serious health risk never to be carelessly courted. Patients and doctors now are finding cause for guarded optimism in two areas of progress linked to drug design and development: a sharp reduction in the number of daily doses of medications most AIDS patients have to take, and new drugs and treatment approaches nearing or in clinical trials. Researchers at the Washington University AIDS Clinical Trials Unit (ACTU), led by director David B. Clifford, MD, are working closely with AIDS patients to move forward with a program of research that respects both the dignity and wishes of the patient and the priorities of physician-scientists. The cornerstone of treatment for HIV/AIDS — the widely used drug "cocktail" — has quietly but dramatically mutated. AIDS patient George Dowling says that he now takes just five pills each day to control the virus, down from a considerably larger number just a few years ago. According to Clifford, who is the Melba and Forest Seay Professor of Clinical Neuropharmacology in Neurology, the decrease in necessary AIDS medications is good news for patients like Dowling because it decreases the chances that patients will miss a dose. That's important, because it limits the HIV virus' opportunity to mutate and become drug-resistant.
David B. Clifford, MD, collects spinal fluid to assess HIV activity within the blood-brain barrier. "Patients do have fewer pills to take, but there are no cures yet; treatment is lifelong and still very costly, and the pills bring with them many unpleasant side effects, some of which in the long term may be life-threatening," says Clifford. Dowling, who participates in a clinical trial at the ACTU, agrees, emphasizing: "The last thing I want to do is to give people the impression that HIV treatment is now a matter of popping a few pills a day and therefore they no longer need to practice prevention." Dowling has been in "remission" from AIDS for approximately seven years. While he once had clinical AIDS and was hospitalized for treatment, he no longer meets any of the conditions that define the disease. His status has been made possible by a mixture of redesigned versions of old and new drugs. Both have been formulated to stay in the body longer, either via larger per-pill doses, gradual release into the body over an extended period of time, or biochemical features that slow their clearance from the body. While drug developers have been getting better at producing AIDS medications that stay in the body longer and are somewhat easier to tolerate, many drugs still have unpleasant side effects. These include cosmetic problems (some AIDS drugs melt away subcutaneous facial fat), gastrointestinal discomfort, sleep loss and abnormal dreams, and chronic fatigue. Researchers also are becoming aware of long-term metabolic side effects of AIDS medications that may potentially be more serious, including dramatically increased risk of cardiovascular disease, insulin resistance and diabetes. "Some of the newer AIDS drugs seem to be able to retain their potency with fewer of these metabolic problems, but for now we have studies underway to see if we can come up with ways to control such dangerous side effects," Clifford says. For Dowling, future unknown drug side effects are not a primary concern. "It's an easy choice to make, because I have to find ways to live with the virus now, and that's a big job," he says. "If there are serious long-term side effects 10 years from now, I'll deal with them 10 years from now." Clinical trials are now underway or coming soon for new classes of AIDS drugs, including entry inhibitors and integrase inhibitors (see "Inhibiting HIV" PDF). Clifford is excited by the potential of these drugs to open up new fronts in the war on HIV. Entry inhibitors seem to be potent even against strains of the virus that are resistant to earlier drugs, but currently approved entry inhibitors have to be administered by injection. The inhibitor Fuzeon™ is a key component of a multicenter trial to see if aggressive early treatment of HIV can more thoroughly eradicate latent copies of the virus that until now have made a cure impossible. "We hope this new approach will be such a potent combination that the latent copies of HIV possibly could decay faster than what we see now with standard therapy," says Lisa A. Mahnke, MD, PhD, a principal investigator who oversees the ACTU's participation in the trial. The ACTU also will soon be involved in trials to see whether patients can be safely treated with just one of the more potent new AIDS drugs, rather than the three types of AIDS drugs that compose most current treatment regimens.
International effort Clifford and his colleagues in the AIDS Clinical Trials Group are leading a major international trial to determine if dosing schedules similar to those in the United States can be used to treat patients in developing nations. Scientists will have to be on guard for genetic differences in other nations that alter patients' responses to medications, and economic feasibility is a major concern. "There's good evidence to think that some of our most potent new drugs may be strong enough to do this," Clifford says. "And that may let us save back some of our ammunition against the possibility that the virus may one day develop resistance to the drug currently in use." The effort to develop a vaccine to prevent HIV infection, which is not a research focus for the ACTU, has not fared well in recent years, according to Clifford. But ACTU researchers are involved in trials of two new ideas for using vaccines to help patients already infected with HIV. One such approach would use existing vaccines for other diseases, such as smallpox or hepatitis, to boost immunity in AIDS patients. Another hopes to use a therapeutic vaccine to reduce the amount of virus in patients' bloodstreams, either as a supplement to regular AIDS treatment or to delay the time when patients with latent HIV have to begin taking AIDS medications. Many challenges and uncertainties lie ahead in the battle with HIV, but as researchers continue to identify new avenues of attack and clinicians develop approaches to ease the burdens of treatment, the virus' seeming invincibility is beginning to falter.
|
||||||