|
|
||
|
Making Filariasis History Eradicating a disfiguring disease one nation at a time
|
|||||||
|
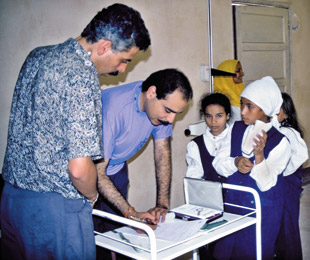
BETTERING PUBLIC HEALTH Gary J. Weil, MD, tests for filariasis in Egypt.
"Filariasis is not as important a disease as AIDS, tuberculosis or malaria, but we don't have the tools to eliminate those diseases yet. We now have the technology and the focus to make an effort globally against filariasis." |
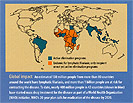
A focused, five-year Egyptian public health campaign has dealt a stinging defeat to lymphatic filariasis, a mosquito-borne parasitic disease that devastates the lives of millions of people worldwide and is a leading cause of disability in many developing countries. The effort is part of a comprehensive strategy to eliminate filariasis from the planet by the year 2020. Gary J. Weil, MD, professor of medicine and of molecular microbiology, has been a major contributor to the campaign. He hopes to see the program's success in Egypt repeated in many other countries. "The world faces many challenges in bringing this kind of campaign to the many nations that are afflicted by this parasite," says Weil, "but our assessment of one of the first national elimination programs is very encouraging."
NATIONAL COMMITMENT Egyptian health care workers dispense antifilarial drugs to those people living in affected regions. Egypt's campaign to eliminate filariasis A systematic program of mapping the affected areas, MDA and follow-up testing has resulted in a sharp decline in infection rates and eliminated the disease in most areas of the country. "The drugs are free or inexpensive, but distribution on this scale in poor agricultural villages is a big, expensive job," Weil says. "Donations from foundations and wealthy countries helped fund the distribution in Egypt, and more of that support is needed for campaigns in other countries." Collaborating with Washington University colleagues including William D. Shannon, PhD, associate professor of biostatistics, and Ramakrishna Rao, PhD, associate research professor of medicine, along with researchers at Ain Shams University in Egypt, Weil developed a plan to assess the Egyptian MDA program's impact. Using several tests, some of which were developed in Weil's lab, Egyptian scientists annually assessed infection rates during the MDA program in four villages near Cairo, each with a population of 3,000 to 5,000 people. The tests revealed sharply declining infection rates in people and in mosquitoes over the course of the program. Weil's filariasis research has kept him traveling to Egypt regularly for nearly two decades. He has high praise for the Egyptian Ministry of Health and Population's efforts to encourage participation in the MDA program, noting the diverse array of economic, cultural and logistical obstacles it has faced in the process. Creative approaches, such as educational comic books for children and television advertisements featuring Egyptian celebrities to promote public awareness, have proved particularly helpful to the effort. A painful scourge, a simple test But coping with the physical problems these conditions create is only half the battle — those afflicted also must deal with the debilitating psychological impact of the disease. "In addition to causing disability, the disfigurement created by elephantiasis is often a source of great social stigmatization," says Weil. Weil has worked for many years to develop improved methods for detecting filarial infections. Filarial worms are transmitted as 1 mm larvae by mosquitoes. They mature in the body to become adult worms over a period of months, then live for years in lymphatic vessels, releasing thousands of microfilariae, microscopic larvae that circulate in the blood until taken up by mosquitoes to begin the cycle anew. Microfilariae hide in the liver and lung during the day when a person is active and can only be seen if blood is collected at night and examined under a microscope — a task difficult to accomplish on a large scale in tropical countries where filariasis is common. Weil realized that an affordable, rapid field test could have a dramatic impact on filariasis control efforts, and he set about developing a method that would detect the worms during the day or night by identifying waste products of the worm in the blood. Because filarial worms in humans are close relatives of the heartworm parasite that infects dogs, Weil first devised a test for heartworm infections. Dog parasites are large and live right in the heart chambers, which made it feasible to develop a test based on detection of worm excretion products. From that experience, Weil's lab moved on to develop a test for filariasis in humans. It works much like a home pregnancy test; instead of urine, however, a drop of blood is placed on a card. The test is read after 10 minutes: A single line means that the person is not infected and that the test is working properly; two lines appear if the person is infected.
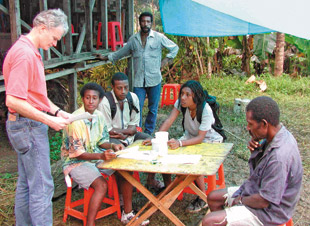
FROM EGYPT TO THE EQUATOR Fresh from the success of the effort in Egypt, Weil's focus now turns to the WHO project's next target for eradication of filariasis, Papua New Guinea. The country's tropical climate and lack of standardized health care will present different challenges. Hope in sight First, filarial worms are believed to live only in humans and mosquitoes. If they lived in another animal host, that species could provide a source of parasites to renew the cycle of human/mosquito infections after an MDA campaign ended it. Second, the worms are inefficiently transmitted. Because they are deposited on the skin and then must crawl into the hole left by the mosquito bite, they need many chances to actually get into a host and start a new infection. This led scientists to theorize that all filariasis in a region wouldn't have to be cured to get the worms to die out. Many experts believe that this will happen if infection rates drop below 1 percent. Finally, the worms are vulnerable to three types of drugs. Manufacturers GlaxoSmithKline and Merck & Co. donate their products for filariasis elimination campaigns, while a third drug is available at an affordable rate. A single dose clears microfilariae from the blood for about one year. But repeated doses are needed, because available treatments are only partially effective against adult worms. Comparing the filariasis eradication effort to the smallpox campaign of the 20th century, Weil notes that the technology for eliminating smallpox — the vaccine developed from a related, but much weaker, virus (cowpox) — was developed in the late 18th century. "It took almost 200 years for public health officials to develop and implement a global eradication program based on this simple tool," he notes, calling the effort one of the most important medical achievements in history. Worldwide effort under way Weil and his colleagues were awarded a grant from the National Institutes of Health's International Collaborations in Infectious Diseases Research program for expanded studies of the results of the Egyptian filariasis elimination program. "We will work with the Ain Shams University group to monitor 44 Egyptian villages and towns, checking to see if remaining infections die out as expected, or if the parasite shows any signs of resurgence," he says. "We'll also be looking at the goals WHO has set for these programs in terms of how far we need to drive infection rates down to eliminate the disease." The success of Egypt's MDA program shows it is possible to eliminate filariasis. However, each country striving to emulate Egypt's success will face its own set of challenges. Not all will have a strong health care infrastructure. Other factors, such as a country's geography and climate, as well as the culture of its people, will also play a role in the successful implementation of a disease elimination campaign. Planners will apply what they have learned in Egypt to maximize the effects of MDA in other nations. Weil, who admitted in a profile published seven years ago that he "mostly had traded [youthful] naive optimism for humility and realism," is feeling a renewed surge of optimism. "I consider myself very fortunate," he says. "Research advances from my laboratory have had a significant impact on this important global public health project."
|
||||||