|
|
||
|
Finding New Ways to Alleviate COPD
|
||||||
|
A new research center will investigate ways to mitigate this growing cause of death. "Try taking a deep breath and then another without exhaling the first, and you'll get an idea of how it feels to have emphysema." |
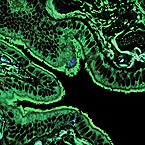
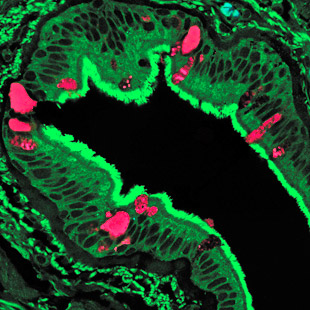
It's a relentless and subtle thief that slowly steals its victims' breath away. It affects about 24 million Americans and is a major cause of disability and death. It's COPD, chronic obstructive pulmonary disease, a lung condition that includes both emphysema and chronic bronchitis. Below: Lung tissue from a patient with COPD highlights cells (pink) producing excess mucus, a symptom of the disease. Left: Normal lung tissue, by comparison, lacks this characteristic.
"COPD is the only leading cause of death that is increasing instead of decreasing," says Michael J. Holtzman, MD, the Selma and Herman Seldin Professor of Medicine and director of the Division of Pulmonary and Critical Care Medicine. "In the next 10 years, it's projected to rise from the fourth to the third leading cause of death in the United States." In COPD, delicate air sacs in the lungs break down and the lung's air passages become clogged because of inflammatory processes and excess mucus production. Right now no cure exists for the disorder, and no therapy will completely halt its progression. "COPD is a slowly progressive disease, with occasional flare-ups, and it's often not recognized in the early stages," says Roger D. Yusen, MD, assistant professor of medicine. "Patients may attribute symptoms like shortness of breath and fatigue to being overweight or getting older, so about half of people with COPD remain undiagnosed." Pioneers in the treatment of COPD, physicians and researchers have launched an all-out effort to uncover new ways to alleviate COPD's symptoms and to find a cure. Treating COPD When these measures aren't sufficient, COPD patients may need supplemental oxygen or surgical procedures such as lung-volume reduction or lung transplantation. Yusen is an investigator in a multicenter study sponsored by the National Heart, Lung and Blood Institute to find out whether giving oxygen therapy earlier in the course of the disease will help patients be more active and live longer. "Low oxygen levels have harmful effects on neurological and cardiac function," Yusen says. "This study will help confirm if there's a survival benefit to oxygen supplementation and also will analyze health care costs and patients' quality of life during long-term oxygen treatment." Washington University surgeons at Barnes-Jewish Hospital developed lung-volume reduction surgery (LVR) in 1993 to counteract one of the characteristic manifestations of COPD — a distended chest cavity caused by air trapped in the lungs. "Try taking a deep breath and then another without exhaling the first, and you'll get an idea of how it feels to have emphysema," says Bryan F. Meyers, MD, associate professor of cardiothoracic surgery. "With the expansion of the lungs and chest, patients don't have much ability to move air in and out." Usually during lung-volume reduction surgery, surgeons remove 20 to 30 percent of lung tissue on each side of the chest. This creates space for the ribs to return to a more normal position and the diaphragm to relax back to its upward curvature so that patients can breathe more freely. Some COPD patients aren't good candidates for bilateral LVR surgery because of a previous surgery or a heart condition. A recent study that Meyers and Yusen conducted found that one-sided or unilateral lung-volume reduction could help such patients. As a potential alternative to lung-volume reduction surgery, endoscopic procedures, which Yusen is studying, close off diseased portions of lungs using inserted valves or a compound that collapses airways. And for COPD patients who have extremely low lung function, transplantation can be considered. "On average, lung transplantation improves quality of life enough to make its associated risks worthwhile for well-qualified patients, and for some patients, lung transplantation improves survival," Yusen says. Yusen is also helping investigate a new drug called roflumilast, which has shown some promise in reducing lung inflammation, and other drugs are under review. "There are a lot of new medications in the pipeline that will allow us to approach COPD from a variety of angles in the future," Yusen says.
Better understanding of COPD can lead to treatments that could halt or even cure the disease. Surgeons Roger D. Yusen, MD, left, medical director of the Lung Volume Reduction Surgery Program, and Bryan F. Meyers, MD, surgical director, meet with patient Howard Wilson to discuss his progress. Researching the cause "When you look at lung tissue from COPD sufferers under the microscope, you see that the usual lattice-like structure has been destroyed," Holtzman says. "One of our projects compares normal and diseased lung tissue and correlates the damage we see in microscopic images to gene expression at the same sites." Finding that some genes are highly active where lung damage is most severe could implicate those genes in the destructive processes of COPD and lead to new treatment targets. The availability of tissue from the lung transplantation program at the School of Medicine aids this research, as do new MRI and CT imaging techniques developed at the university. "Outside of our laboratories, very few places in the world have the combination of technology, expertise and clinical material to do the studies we are undertaking," Holtzman says. Researchers in Holtzman's group also are investigating abnormalities in genes that produce elastin, a protein in the lung's air sacs that gives them their ability to stretch and spring back. Additional projects analyze why certain enzymes in COPD lung tissue chew up structural proteins like elastin and its cousin, collagen, which can lead to scarring of the lungs. As lung tissue breaks down, chronic inflammation makes things even worse. But the specific inflammatory and immune factors causing COPD are only now being identified. Holtzman and his colleagues discovered that, in response to inflammation and immune system components, the airways of COPD sufferers accumulate too many mucus-producing cells, which contribute to airway obstruction. "At this time, no drugs specifically counteract overproduction of mucus," Holtzman says. "One of our goals is to understand how excess mucus cells develop. Then we can target these precursor stem cells and alleviate some of the symptoms of airway obstruction." From work with children who experience severe respiratory infections, Holtzman has found that viruses also may play a role in COPD development, especially if people already have certain genetic predispositions. "Using mice that develop a condition that mimics COPD, we've found that a kind of cellular reprogramming occurs after viral infection that makes the animal more sensitive to inhaled stimuli like cigarette smoke," Holtzman explains. "We hypothesize that a similar thing happens with people. You start with a genetic susceptibility, get a certain type of viral infection as a child, and then if you smoke you go further down the path toward COPD." His research group also is delving into experiments that show lung tissue can regrow under some conditions. "We're beginning to appreciate that lung tissue is constantly being destroyed and regenerated in the process of this disease," Holtzman says. "That finding offers the possibility that in the future we may be able to alter the regeneration process to reverse some of the effects of COPD."
|
|||||