Washington University researchers are leaders in efforts to learn how deep-brain stimulators affect the brain and how to fine-tune the installation and application of stimulators in order to maximize benefits and minimize side effects.
And those efforts are just one branch of a multidisciplinary campaign that is moving forward on multiple fronts in the battle against Parkinson’s.
While he’s pleased with the progress many patients are making with DBS, Joel S. Perlmutter, MD, head of the Movement Disorders Section in the Department of Neurology, is careful to emphasize that it’s an option to be considered only after the many different possible medication regimes for controlling Parkinson’s disease have failed.

Joel S. Perlmutter, MD
“As a doctor advising patients, I say, ‘If the pills work, don’t put two holes in your head,’” says Perlmutter, who also is professor of neurology, neurobiology, physical therapy, occupational therapy and radiology. “Surgery has serious risks, and maintenance of the implants also requires us to operate again years later to replace the batteries.
Perlmutter talks in quiet, soothing tones that contrast with the boundless energy and no-nonsense attitude he brings to patient care and research. Although initially highly skeptical of DBS, the evidence won him over.
He estimates 10 to 20 percent of Parkinson’s patients eventually go on DBS. Approximately 75 DBS installation surgeries are performed each year at Barnes-Jewish Hospital.
The program is led by physician Samer D. Tabbal, MD, associate professor of neurology, and surgeons Keith M. Rich, MD, professor of neurosurgery, radiation oncology and neurobiology, and Joshua L. Dowling, MD, associate professor of neurological surgery.
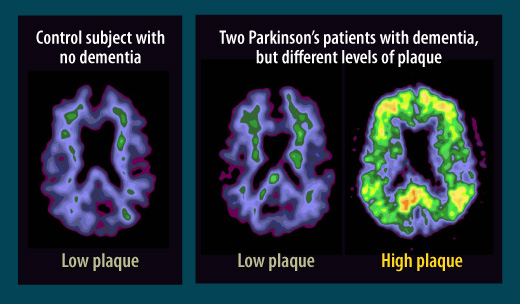
“Dementia and other cognitive problems are the biggest unmet need in Parkinson’s disease, now that we have DBS.”
— Joel S. Perlmutter, MD
How does DBS help? Thanks in part to studies by Perlmutter, Tamara G. Hershey, PhD, associate professor of psychiatry, neurology and radiology, and Kevin J. Black, MD, professor of psychiatry, neurology, radiology and neurobiology, scientists know that current from the DBS causes increased activity in regions of the brain connected to the subthalamic nucleus.
“If Parkinson’s is like getting persistent crank calls in the middle of the night on your bedroom phone, the deep brain stimulator is like taking that phone off the receiver and setting it on the table,” Perlmutter explains. “We believe the DBS causes the neurons to fire often enough that the abnormal firing patterns caused by Parkinson’s disease can’t get through.”
Precise placement
For many patients like Susan Tinzmann, this brings significant improvements in their ability to move and walk. For some, though, it also can bring impairments in higher cognitive functions. Patients can drive a car or play golf again, but they might not be able to program a computer or may experience trouble with their moods or their speech.
Could the placement of the electrodes be making a difference? Spurred in part by evidence that the subthalamic nucleus may have distinct functional areas, Tom O. Videen, PhD, research professor of radiology and neurology, Morvarid Karimi, MD, assistant professor of neurology, and others developed a method for much more precise assessment of where the DBS contacts are placed in the brain.
“We knew where the electrodes were going within a couple of millimeters, which was good enough for patient care,” Perlmutter explains, “but it wasn’t telling us what precise parts of the subthalamic nucleus were receiving the current and linking those parts to good results or side effects.”
The new approach to assessing electrode placement can only be definitively confirmed via autopsies of patients who had DBS implants, an effort that’s under way now. But after initial tests tentatively validated the method, Hershey and colleagues used it to show that stimulating the lower side of the subthalamic nucleus impaired a cognitive function known as response inhibition, which is important for impulse control and adaptive behavior.
“On another front, we had thought improvement in movement would mostly come from stimulating the top part of the subthalamic nucleus, but it turns out that effect is a kind of like a hand grenade,” Perlmutter says. “We could miss the subthalamic nucleus entirely and still get motor benefit.”
Researchers are now working to use brain scans to link stimulation of particular parts of the subthalamic nucleus to increases in activity in other parts of the brain. They hope to eventually produce a map of the subthalamic nucleus that highlights the areas where DBS impulses can do the most good while causing the fewest side effects.