|
|
||
|
DNA Rx Cancer prescriptions are written in genetic code.
|
|||||||
|
“Until now, clinicians treated everyone the same
way. In this unique project, we’re actually acting on data prospectively
to see if we can individualize treatment.”
“Results from our studies of colorectal cancer will
help us think about how we can begin to apply pharmacogenetics to other
tumor types.”
“Pharmacogenetics lets us individualize this treatment,
which is a prelude to surgery. We hope
|
THE WAITING REALLY WAS THE HARDEST PART for researcher Howard L. McLeod, PharmD. As a specialist in pharmacogenetics, the study of interactions between drug treatments and an individual’s genetic code, McLeod could see a day coming when doctors would use their patients’ genes to steer them away from potentially hazardous reactions to medications and toward beneficial outcomes. But that day didn’t seem to be getting any closer. “It seemed like the best estimate was always that it would be another 10 years before we could put these kinds of approaches to use,” says McLeod. “Those 10 years just never seemed to end.” About two years ago, McLeod decided he’d had enough waiting. With colleagues in several departments at the School of Medicine and Barnes-Jewish Hospital, he put together the first study in the United States that uses patients’ genetic information to modify their treatments. Now about halfway finished, the study focuses on colorectal cancer patients and a gene that appears to be linked to how positively patients respond to chemotherapy and radiation treatments. Patients with a form of the gene that decreases their chances of having a good response are given added chemotherapy.
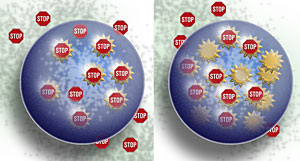
Cancerous cells from patient A (left): A standard dose of chemotherapy blocks the activity of a key protein, making tumor cells more vulnerable to radiation treatments. Cancerous cells from patient B (right): Because of genetic differences, this patient’s tumor cells produce more of the key protein, overwhelming the standard drug. Physicians give this patient a second chemotherapeutic agent to make sure the protein’s fortifying effects are blocked. “Until now, clinicians treated everyone the same way and then scientists looked back and said, ‘Hey, by the way, this patient population A, with this particular set of genes, has a better response to the treatment; or patient population B, with these genes, has more toxicity,’” says Benjamin R. Tan, MD, a medical oncologist and assistant professor of medicine who is involved in the study. “In this unique project, though, we’re actually acting on that data prospectively to see if we can individualize treatment.” When he talks about using pharmacogenetics to modify patient treatment, McLeod, associate professor of medicine, genetics, and of molecular biology and pharmacology, sparkles with energy, wit and enthusiasm. “The basic concepts behind pharmacogenetics have been around forever,” says McLeod, who also directs the Pharmacology Core at the Alvin J. Siteman Cancer Center. “I like to say that the quest to find out who’s going to get toxicity and who’s going to benefit from medicine has been around since we’ve been chewing bark. But now we have the technology to actually put these ideas to use.” To generate leads for genes that might potentially interact with a drug, a phase of pharmacogenetics that McLeod refers to as “stamp collecting,” scientists first assemble a detailed list of the key proteins known to interact with a drug. Researchers can typically put together a list of several proteins that interact with most drugs, including enzymes known to activate or degrade the drug, take it into or out of cells, or help distribute it around the body or speed its exit from the body. Pharmacogeneticists then check if changes in the genes for those proteins seem to correlate with changed treatment outcomes. “The good side is that it’s a very educated guess, and the bad side is that it’s still a guess,” McLeod says. “But it’s still much better than searching all 35,000 genes in the human genome.” McLeod and the researchers in his laboratory follow up on early leads generated by other labs, searching through larger and more tightly controlled pools of patient data to see if the leads check out. With support from the National Cancer Institute, McLeod’s research group recently conducted a review of several genetic markers tentatively linked to effects on colorectal cancer treatment. “So far, we’re finding that the majority of markers that are in the literature do not validate — they have no relationship with toxicity or effectiveness when examined in a larger patient population,” McLeod says. “But there are markers that are true, markers where we have very clear data showing they were associated with either risk of severe toxicity or the chance of having a therapeutic response to the medicines.”
Multidisciplinary medicine can lead to better treatments and improved survival rates for patients. McLeod is delighted that colorectal cancer is the focus of the first applied pharmacogenetics study. He feels this tumor type has been shortchanged in terms of public attention because it primarily affects older patients and because it occurs in an area of the body no one likes to talk about. “Results from our studies of colorectal cancer will help us think about how we can begin to apply pharmacogenetics to other tumor types including lung, breast and prostate cancers,” he says. McLeod notes that more than one gene is known to contribute to colorectal cancer, so a thorough pharmacogenetic approach to managing treatment will inevitably have to consider the potential effects on treatment of several different genes. And in the end, genetics is unlikely to account for all variability in patient responses to treatment. McLeod estimates that as much as 50 percent of that variability may stem from other factors, such as a patient’s diet. Understanding these contributors to variability becomes a priority as more options for treatment become available. For 40 years, physicians had only one approved chemotherapy drug for colorectal cancers, but in recent years four new drugs have been introduced. “Now that we have five drugs, how do we decide what to do? We have to find out information from our patients and their DNA to determine which drug will be most likely to give them the best results,” McLeod says. Treatment for patients with colorectal cancer begins with chemotherapy and radiation. “Pharmacogenetics lets us individualize this treatment, which is a prelude to surgery,” says Robert S. Malyapa, MD, PhD, assistant professor of radiation oncology. “We hope that this will have a positive effect on both tumor control and long-term survival.” Malyapa, who specializes in radiation treatment for gastrointestinal tumors at the Siteman Cancer Center, explains to patients the treatment recommendations and options, including potential participation in clinical trials. He finds that patients given the option of participating in the pharmacogenetics trial are usually quite eager to do so because it may directly benefit them. When patients agree to participate, a clinical trial coordinator takes a blood sample scientists use for DNA analysis. They look at a gene in the patient’s DNA that can affect how much the patient’s cells make of a protein, thymidylate synthase (TS), that is the primary target for a major chemotherapy drug, 5-fluorouracil. Several laboratories earlier found that patients with high levels of the TS protein or of the RNA for making the protein typically did not respond well to chemotherapy. “Physicians can only give a certain amount of When they detect the form of the gene that increases production of TS, clinicians add a second chemotherapy agent to improve their chances of seeing tumors shrink prior to surgery.
What kind of patient are you? Your individual genetic
code may help determine the best treatment options “This is pure translational research — really,
what everyone is striving to do more of now,” comments David W.
Dietz, MD, a colorectal surgeon involved Though it was conceived before the university officially announced its BioMed 21 initiative, the pharmacogenetics trial includes many of the key elements that BioMed 21 seeks to encourage in research: it brings the latest in basic research to bear on patient care, it makes use of the new wealth of human genetic data now available, and it involves collaboration across several departments. “This is really an example of multidisciplinary medicine at its best,” McLeod says. “We could never do this study if the radiation oncologists, medical oncologists, surgeons, radiologists and pathologists weren’t all 100 percent on board.” McLeod anticipates that the study will finish early next spring. He’s not making any promises on how far that first step will take pharmacogenetics researchers, but he’s extremely glad to have finally set that step in motion. “This is not a done deal — this is an evolving,
new way of practicing,” he notes. “But it’s where the
future is, certainly for colon cancer, and I think it’s going to
be the future for all cancers.”
|
||||||