




A year and a half after the first COVID-19 shutdowns in the U.S. transformed life as we know it, the end to the pandemic is nowhere in sight. Masking and distancing can bring case numbers down, but at an economic and social cost many find intolerably high. Scientists developed fantastically effective vaccines in record time, but officials failed to get shots into arms fast enough to prevent a devastating fourth wave in the U.S.
For the physicians and scientists at the School of Medicine, reining in COVID-19 has been an ever-changing struggle. In the first, desperate months, they dove into the global race to find treatments, diagnostics and vaccines. Later, attention shifted toward understanding the long tail of COVID-19 symptoms, monitoring the threat of new virus variants, studying racial inequities and optimizing vaccination strategies.
Experts predict that mass vaccination eventually will end the pandemic but won’t eradicate the virus. We will just have to learn to live with it, they say. But the insights into human biology and behavior gleaned from this extraordinary time also will stay with us, informing medical care as we all adapt to the new normal.

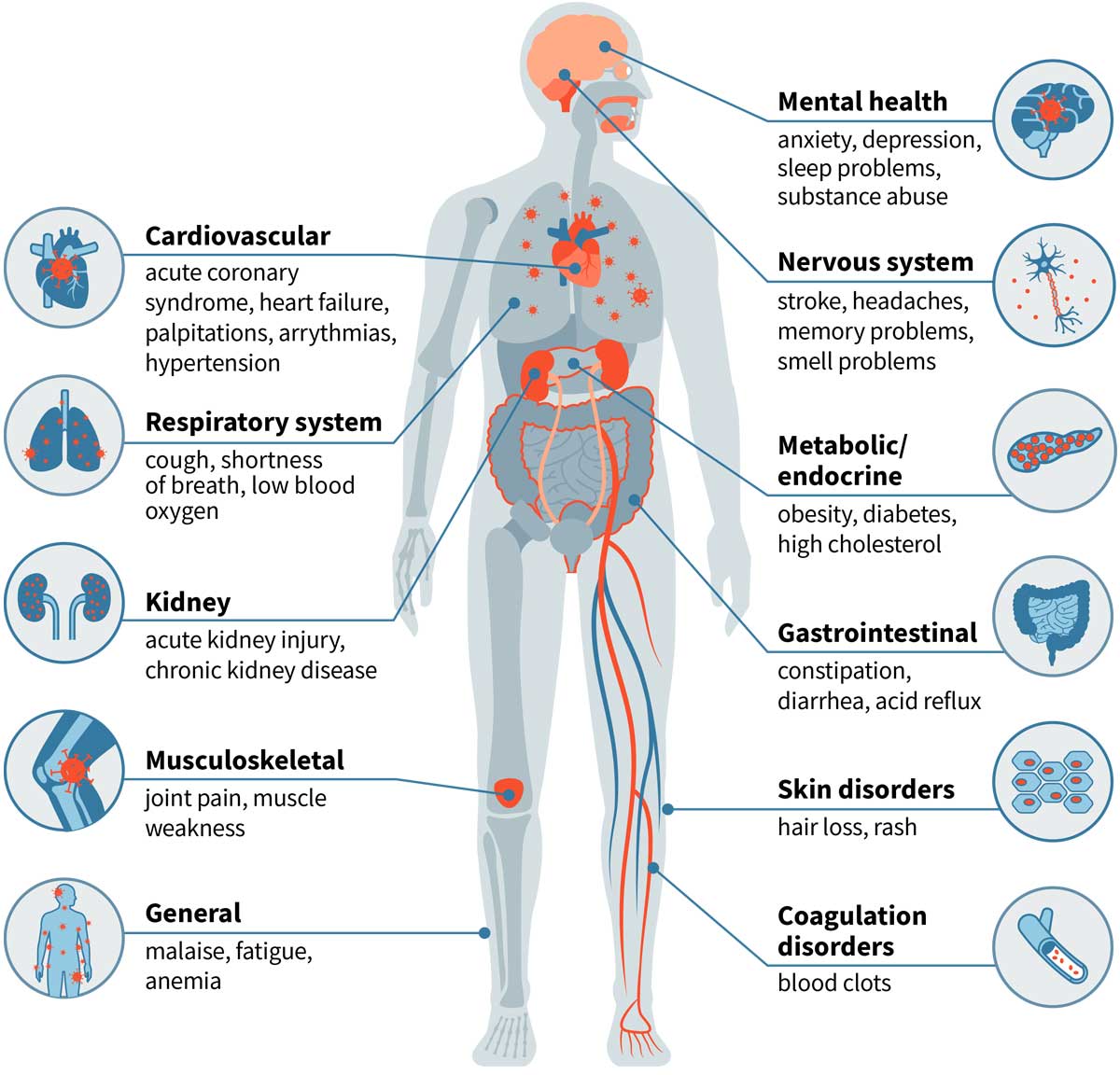
The long tail of COVID-19
Some people survive COVID-19 but don’t fully recover for months, if at all. School of Medicine researchers are investigating why the effects of COVID-19 can linger long after the virus is gone.
Still at risk
Even people with mild cases of COVID-19 are at increased risk of death for months after the acute illness has passed, according to a study by Ziyad Al-Aly, MD, a kidney doctor who specializes in big data. By analyzing thousands of veterans’ health records, Al-Aly found that COVID-19 survivors face nearly a 60% higher chance of death from all causes in the six months after diagnosis. The higher risk of death was linked to persistent major health issues affecting nearly every organ system.
Surviving but not thriving
A third of COVID-19 survivors seek care for a new medical condition in the aftermath of the disease, estimates data scientist Philip R.O. Payne, PhD, based on an ongoing analysis of new patient visits. Heart trouble is among the most common problems. A study by cardiologist Kory J. Lavine, MD, PhD, found that the virus that causes COVID-19 can infect heart muscle and destroy the muscle fibers responsible for contractions, possibly resulting in lasting damage.

The nose knows
A curious symptom of COVID-19 is loss of the sense of smell. Otolaryngologist Jay F. Piccirillo, MD, aims to restore people’s sense of smell by retraining their brains via daily exposure to essential oils. “When we think about loss of smell, we probably think about the inability to appreciate cheese or coffee or wine,” Piccirillo said. “But our patients’ main concern is smelling smoke and natural gas. Their first concern is safety.”

The vaccine race
With multiple COVID-19 vaccines available and the global vaccination effort underway, focus has shifted to understanding how well such vaccines work for special populations and creating better vaccines for current and future pandemics.
A needle-free vaccine
Cancer biologist David T. Curiel, MD, PhD, and Michael Diamond, MD, PhD, a virologist and immunologist, have created an inhaled COVID-19 vaccine that may reduce infection and transmission in addition to preventing severe illness and death. The vaccine is designed to fortify immune defenses in the nose, right where the virus is most likely to land. The vaccine sailed through animal testing and is now in clinical trials in people.

No one left behind
Pregnant women, breastfeeding mothers, and people with certain medical conditions were excluded from COVID-19 vaccine trials, so School of Medicine researchers are stepping up. Ob-gyn Jeannie C. Kelly, MD, found that vaccinated nursing mothers may pass protective antibodies to their babies through breast milk. Rheumatologist Alfred Kim, MD, is evaluating COVID-19 vaccines in people taking immunosuppressive drugs such as the ones for arthritis and lupus.
Does vaccination reduce transmission?
As COVID-19 resurged last summer, the Centers for Disease Control and Prevention recommended that everyone wear masks, regardless of vaccination status. “We know vaccinated people can transmit the virus, but we don’t know how well they transmit it,” said Rachel M. Presti, MD, PhD, director of the Infectious Diseases Clinical Research Unit. Presti is the Washington University site leader for the NIH-led PreventCOVIDU trial. The trial aims to measure transmission by vaccinated and unvaccinated people. Participants will fill out daily questionnaires, take daily nasal swabs over a four-month period, provide blood samples and undergo contact tracing.

Closing the deal
Bringing this virus to heel requires not just having effective vaccines but getting those vaccines into the people who still need them, monitoring how long immunity lasts, and tracking the spread of new virus variants.
Aiming for herd immunity
The St. Louis region is still far from herd immunity, and reaching the remaining unvaccinated people is challenging. Data scientist Philip R.O. Payne, PhD, spent much of 2020 finding local hot spots of disease to track its spread. Now, he has turned his attention to finding cold spots of low vaccine uptake so distribution can be targeted to the communities most at need.

How long does immunity last?
The pandemic nightmare scenario was that COVID-19 immunity induced by disease or vaccination would fade quickly, making herd immunity impossible. Immunologist Ali H. Ellebedy, PhD, helped put those fears to rest. In a pair of papers, he showed that survivors of mild COVID-19 harbored antibody-producing cells nearly a year after infection. Most Pfizer vaccine recipients had laid the foundations for strong, lasting immune responses, even though certain high-risk populations may benefit from a booster after eight months.
Tracking a changeable foe
Virus variants are constantly emerging, and some may be resistant to COVID-19 drugs and vaccines. In a pair of papers, Michael S. Diamond, MD, PhD, showed that while antibodies that work against the original form of the virus tend to be less effective against variants, COVID-19 drugs made from combinations of two antibodies mostly retained effectiveness. “We will have to continue monitoring and be prepared to adjust our vaccines and antibody-based therapeutics if necessary,” Diamond said.

The new normal
When the pandemic recedes, the world will be different. Telemedicine may be here to stay, and possibly masking in winter, too. And the racial inequities laid bare by the pandemic may spur a reassessment of biases in medicine and a move toward better health for all.

Rooting out bias
Black neighborhoods in St. Louis received less COVID-19 testing in the spring and summer of 2020 despite higher hospitalization rates, according to a study by infectious disease specialist Elvin H. Geng, MD. Ongoing studies suggest that Black neighborhoods in the region also have reduced vaccination rates. Racial disparities like these worsen health in minoritized communities and must be systematically addressed, said Will R. Ross, MD, associate dean for diversity.

The doctor is home
The infrastructure for telepsychiatry was underutilized until the pandemic forced a rethinking of traditional practices. “One of the silver linings of the pandemic has been a wholesale conversion of outpatient mental health practice to telehealth,” said child psychiatrist John N. Constantino, MD. “Most patients are very happy with telehealth, especially when necessary for safety or transportation barriers, and with increased efficiency we’re actually delivering more mental health care than before.”

The mask stays on
In-school COVID-19 transmission is rare as long as schools heed public health precautions such as mandatory masking, distancing and frequent hand-washing, according to a CDC study in Missouri and elsewhere.
“The study was done before vaccines were available, so it tells you that prevention strategies work,” said pediatric infectious disease specialist Jason G. Newland, MD, who helped lead the Missouri arm. “Until we have universal vaccination, we can’t stop masking. We need to continue doing what we did last year to protect children and adults in schools.”
 Share
Share Tweet
Tweet Email
EmailPublished in the Autumn 2021 issue